
Introduction
Chronic pain affects an estimated 50 million adults in the United States – roughly 20% of the adult population. For many, non-opioid treatments such as physical therapy, over-the-counter medications, and lifestyle changes provide adequate relief. But for others, pain persists despite these efforts.
This raises a difficult question: When is opioid therapy appropriate for chronic pain?
The answer is not simple. Opioids – including medications like tapentadol, oxycodone, and morphine – are powerful tools, but they carry serious risks of addiction, respiratory depression, and overdose. This educational guide outlines the general principles that guide healthcare providers when considering opioid therapy for chronic pain.
This information is for educational purposes only and does not replace professional medical advice. Always consult a licensed healthcare provider for personalized treatment recommendations.
Understanding Chronic Pain Before Considering Opioids
What Is Chronic Pain?
Chronic pain is defined as pain that persists for longer than three months – often continuing after the initial injury or illness has healed. Unlike acute pain (which serves as a warning signal), chronic pain can become a disease itself, involving changes in the nervous system that amplify pain signals.
The First-Line Approach
Before considering opioid therapy, guidelines from the Centers for Disease Control and Prevention (CDC) , the American Pain Society, and other organizations recommend trying non-opioid treatments first.
First-line treatments for chronic pain include:
| Category | Examples |
|---|---|
| Non-opioid medications | NSAIDs (ibuprofen, naproxen), acetaminophen |
| Neuropathic pain medications | Gabapentin, pregabalin, duloxetine, amitriptyline |
| Physical therapy | Exercise, manual therapy, stretching |
| Psychological approaches | Cognitive behavioral therapy (CBT), mindfulness |
| Interventional procedures | Nerve blocks, epidural injections (for selected conditions) |
| Lifestyle modifications | Weight loss, smoking cessation, sleep hygiene |
💡 Opioids are generally NOT recommended as first-line therapy for chronic pain. They are typically considered only after non-opioid options have been tried and found inadequate.
General Criteria for Considering Opioid Therapy
When non-opioid treatments provide insufficient relief, doctors may consider opioid therapy for chronic pain if the following general criteria are met.
1. Moderate to Severe Pain That Significantly Impairs Function
Opioids are reserved for moderate to severe pain that interferes with daily activities, work, sleep, or quality of life. Mild pain – even if chronic – is generally not treated with opioids.
Signs that pain severity may warrant opioid consideration:
- Pain rated 5 or higher on a 0-10 scale despite non-opioid treatments
- Inability to work or perform daily tasks (dressing, cooking, cleaning)
- Sleep frequently disrupted by pain
- Pain limits social engagement or family activities
2. Failure of Non-Opioid Treatments
Opioid therapy is typically considered only after adequate trials of multiple non-opioid treatments have failed or are not tolerated.
What “failure of non-opioid treatments” generally means:
- At least two different non-opioid medications tried at adequate doses and durations
- A supervised trial of physical therapy (when appropriate)
- Consideration of psychological approaches (CBT, especially for high-risk patients)
- Treatment of underlying conditions (e.g., optimizing diabetes management for neuropathy)
3. No Active Contraindications to Opioid Therapy
Certain conditions make opioid therapy unsafe or inappropriate.
Absolute contraindications (opioids should generally NOT be used):
- Severe respiratory depression
- Acute or severe bronchial asthma (unmonitored setting)
- Known or suspected gastrointestinal obstruction
- Concurrent use of MAO inhibitors (within 14 days)
- Known hypersensitivity to the specific opioid
Relative contraindications (use with extreme caution, if at all):
- History of substance use disorder (active or recent)
- Severe untreated depression or anxiety
- Active suicidal ideation
- Severe sleep apnea (untreated)
- Advanced liver or kidney disease (dose adjustment may not be sufficient)
4. Absence of High-Risk Behaviors or Conditions
Before initiating opioid therapy, doctors assess for risk factors that increase the likelihood of misuse, addiction, or overdose.
Risk factors that may delay or preclude opioid therapy:
- Personal history of opioid or other substance use disorder
- Family history of substance use disorder
- Current or past legal issues related to controlled substances
- Psychiatric conditions (untreated bipolar disorder, psychosis)
- Use of benzodiazepines or other CNS depressants
- Multiple unscheduled “lost” prescriptions or early refill requests
5. Patient Willingness to Participate in Monitoring and Safety Protocols
Opioid therapy requires active participation from the patient.
Typical requirements for ongoing opioid therapy include:
- Agreement to a written treatment agreement (opioid contract)
- Random urine drug testing (to ensure compliance and detect non-prescribed drugs)
- Single prescribing provider and single pharmacy (to prevent “doctor shopping”)
- Regular follow-up appointments (typically every 1-3 months initially)
- Safe storage (locked cabinet) and proper disposal of unused medication
Specific Chronic Pain Conditions Where Opioids May Be Considered
Not all chronic pain conditions are equally responsive to opioids. Research supports opioid therapy for some conditions more than others.
Cancer Pain
Evidence: Strong
Consideration: Opioids are a cornerstone of cancer pain management, especially for moderate to severe pain. Non-opioid options are used alongside opioids (not instead of them when pain is severe).
Chronic Lower Back Pain (Selected Patients)
Evidence: Moderate for short-term relief; limited for long-term (more than 12 months) benefit
Consideration: Opioids may provide meaningful relief for some patients with chronic lower back pain who have failed other treatments. However, benefits often diminish over time, and risks persist. Opioids are not recommended as long-term monotherapy.
Osteoarthritis Pain (Selected Patients)
Evidence: Moderate
Consideration: For patients with severe hip or knee osteoarthritis who are not candidates for surgery (or awaiting surgery) and have failed other treatments, opioids may provide temporary relief. However, non-opioid options (NSAIDs, topical agents, physical therapy, weight loss) remain preferred.
Diabetic Peripheral Neuropathy (Neuropathic Pain)
Evidence: Weak to moderate
Consideration: First-line treatments for diabetic neuropathy are gabapentin, pregabalin, and duloxetine. Tapentadol (due to its dual mechanism) has some evidence for neuropathic pain, but it is generally not first-line.
Fibromyalgia
Evidence: Weak
Consideration: Opioids are generally NOT recommended for fibromyalgia. The FDA-approved treatments for fibromyalgia are pregabalin, duloxetine, and milnacipran. Exercise and CBT are also strongly supported.
Complex Regional Pain Syndrome (CRPS)
Evidence: Limited
Consideration: Some patients with CRPS may benefit from opioids, but evidence is limited. Multidisciplinary care (physical therapy, psychological support, interventional procedures) is preferred.
The Process of Initiating Opioid Therapy (Step-by-Step)
When a doctor and patient decide to try opioid therapy, the process typically follows a structured approach.
Step 1: Baseline Assessment
- Pain assessment – Character, severity (0-10 scale), location, impact on function
- Medical history – Review of contraindications, organ function (liver/kidney), respiratory status
- Mental health screening – Depression, anxiety, substance use disorder risk
- State Prescription Drug Monitoring Program (PDMP) check – To identify potential “doctor shopping”
- Baseline urine drug test – To confirm no unprescribed substances
Step 2: Informed Consent
The doctor explains the risks, benefits, and alternatives. The patient acknowledges understanding. This is often documented with a signed opioid treatment agreement.
Step 3: Starting Low and Going Slow
- Lowest effective starting dose is used (e.g., tapentadol 50mg immediate-release or 50mg extended-release)
- Short-acting (immediate-release) opioids are preferred for initiation, even if the goal is long-acting therapy
- “As needed” (PRN) use is generally not recommended for chronic pain; fixed dosing schedules are preferred
Step 4: Monitoring and Follow-Up
- Reassessment within 1-4 weeks – Evaluate pain relief, function, side effects, and signs of misuse
- Follow-up every 1-3 months for stable patients
- Ongoing PDMP checks (every 3-6 months or as required by state law)
- Periodic urine drug testing (random, at least annually, often more frequently)
Step 5: Reassessment of Risks and Benefits
At each visit, the doctor asks: Is the benefit (pain relief, improved function) worth the risk?
If not – for example, if pain relief is minimal but side effects or concerning behaviors emerge – the doctor may taper and discontinue opioid therapy.
Risks of Long-Term Opioid Therapy (What Patients Should Know)
Understanding the risks is essential before starting or continuing opioid therapy.
Addiction (Opioid Use Disorder)
- Affects an estimated 8-12% of patients on long-term opioid therapy for chronic pain
- Signs include craving, loss of control over use, continued use despite harm, and withdrawal symptoms
- Risk is higher with personal or family history of substance use disorder, psychiatric conditions, and higher doses
Tolerance
- Over time, the same dose provides less pain relief
- May lead to dose escalation (which increases other risks)
- Tolerance to pain relief does NOT develop equally to respiratory depression (dangerous)
Respiratory Depression
- The most serious risk – breathing slows or stops
- Risk is highest during initiation, dose increases, or when combined with alcohol, benzodiazepines, or other CNS depressants
- Fatal overdose is possible, even with prescribed doses
Hyperalgesia (Opioid-Induced Hyperalgesia)
- A paradoxical condition where opioids increase pain sensitivity over time
- May explain why some patients experience worsening pain despite escalating doses
Endocrine Effects
- Opioids can suppress sex hormones, leading to low libido, infertility, depression, and bone loss
Gastrointestinal Effects
- Constipation is extremely common and does not improve with tolerance
- May require proactive treatment with stool softeners, laxatives, or peripherally acting opioid antagonists (e.g., naloxegol)
Accidental Overdose and Death
- Risk increases with higher doses (especially >50 morphine milligram equivalents per day)
- Risk increases with concurrent benzodiazepine use (avoid combination whenever possible)
Alternative Approaches Before Opioids – Worth Revisiting
Before accepting opioid therapy, consider whether these options have been adequately tried.
| Modality | How to Access | Typical Trial Duration |
|---|---|---|
| Physical therapy | Referral from primary care | 6-12 weeks |
| Cognitive behavioral therapy (CBT) | Psychologist, social worker, or online program | 8-12 sessions |
| Pain psychology | Pain management center | Variable |
| Acupuncture | Licensed acupuncturist | 6-12 sessions |
| Yoga or tai chi | Community classes or online | 8+ weeks |
| Exercise program | Physical therapist or personal trainer | Ongoing |
| Medication review | Pharmacist or prescribing doctor | Immediate |
| Sleep optimization | Sleep specialist or CBT for insomnia | 4-8 weeks |
💡 Many patients find that a combination of these approaches – not just medications – provides the best long-term outcomes.
Special Considerations for Tapentadol in Chronic Pain
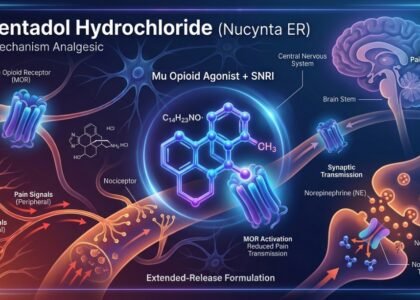
Tapentadol (available in the USA as Nucynta® and internationally as Aspadol, Tapaday, Palexia, and other brands) has some unique features that may influence treatment decisions.
Advantages of Tapentadol for Certain Patients
- Dual mechanism – May be more effective for mixed pain (nociceptive + neuropathic) than traditional opioids
- Lower rates of certain side effects – Some studies suggest less nausea and constipation compared to oxycodone
- No active metabolites – May be safer in patients with liver or kidney impairment (though dose adjustment is still needed)
When Tapentadol May Be Considered
- Chronic lower back pain with a neuropathic component
- Diabetic peripheral neuropathy (when first-line treatments are inadequate or not tolerated)
- Osteoarthritis pain with significant functional impairment in patients who cannot take NSAIDs
Important Limitations
- Tapentadol is a Schedule II controlled substance with high abuse potential
- Extended-release Tapentadol is only for around-the-clock pain, not “as needed” use
- Higher strengths (150mg, 200mg, 250mg) are for opioid-tolerant patients only
Frequently Asked Questions (FAQs)
Q1. Are opioids ever first-line treatment for chronic pain?
Rarely. Opioids are generally not first-line for any chronic pain condition except cancer pain, end-of-life care, and acute severe pain. For non-cancer chronic pain, non-opioid treatments should be tried first.
Q2. How long can someone safely take opioids for chronic pain?
There is no simple answer. Some patients with severe, refractory pain (e.g., certain cancer survivors, select patients with failed back surgery syndrome) may remain on stable, low-dose opioids for years under close monitoring. However, risks increase with duration. Many guidelines suggest reassessing the risk-benefit ratio at least annually.
Q3. What is the safest opioid for chronic pain?
No opioid is “safe” – all carry risks. However, some have features that may reduce certain risks:
- Tapentadol or tramadol – Dual mechanism may allow lower opioid receptor activation
- Buprenorphine – Partial agonist with a “ceiling effect” for respiratory depression (used off-label for chronic pain)
- Morphine, oxycodone, hydrocodone – Traditional opioids with well-understood profiles
Your doctor will choose based on your specific condition, other medications, and risk factors.
Q4. Can I take opioids as needed (PRN) for chronic pain?
For chronic pain requiring around-the-clock treatment, fixed dosing is preferred to avoid “breakthrough” pain cycles. “As needed” use is generally reserved for acute pain or occasional breakthrough pain in patients already on long-acting opioids.
Q5. What should I do if I think I am becoming addicted to my pain medication?
Speak with your doctor immediately. Do not stop opioids suddenly (withdrawal can be severe and dangerous). Your doctor can help with:
- Tapering off opioids safely
- Referring to addiction specialists or medication-assisted treatment (buprenorphine, methadone, naltrexone)
- Transitioning to non-opioid pain treatments
Q6. Will my doctor stop prescribing opioids if I use medical marijuana?
It depends on your doctor, state laws, and the specific situation. Many doctors will not prescribe opioids to patients using cannabis due to lack of safety data, potential for increased sedation, and legal complexities. Be honest with your doctor about all substances you use.
Q7. Can I drive while taking opioids for chronic pain?
Generally, no. Most opioids cause drowsiness, dizziness, and impaired reaction time. Driving is discouraged, especially during the first few weeks of treatment or after any dose increase. Your doctor can provide specific guidance based on your response to the medication.
Conclusion
Opioid therapy for chronic pain is a serious decision with lifelong implications. It is not a first-line treatment and should only be considered after adequate trials of non-opioid medications, physical therapy, psychological approaches, and lifestyle modifications.
When opioid therapy is appropriate – for patients with moderate to severe chronic pain who have failed other treatments and are at low risk for misuse – it should be prescribed at the lowest effective dose, with the shortest duration possible, and under close, ongoing monitoring.
For patients who require opioid therapy, medications like tapentadol may offer unique advantages due to their dual mechanism of action. However, all opioids carry significant risks, including addiction, respiratory depression, and fatal overdose.
The decision to start opioid therapy should be shared, informed, and revisited regularly. If you are living with chronic pain, talk with your healthcare provider about the full range of options – both opioid and non-opioid – to develop a personalized pain management plan that maximizes benefit while minimizing risk.
📌 Key takeaway: Opioids are powerful tools for selected patients with chronic pain, but they are not a cure. The goal is improved function and quality of life – not complete pain elimination. Non-opioid approaches remain the foundation of chronic pain management.
🚨 This content is for educational and informational purposes only. Tapentadol.org does not provide medical advice, diagnosis, or treatment. Always consult a licensed healthcare provider for medical concerns. If you are experiencing a medical emergency, call 911 immediately.